In a 2025 blog, Dr Dimitrios Panayotopoulos-Tsiros examines how community-based initiatives such as walking groups, workshops and peer networks help men build trust, purpose and social connection. Drawing on ongoing research with the Centre for Policy Research on Men and Boys, he explores where this support infrastructure exists, where gaps remain, and how policy can strengthen it without undermining the trust that makes it effective.

The government’s recently published Men’s Health Strategy places men’s health within a broader shift from sickness to prevention and recognises that further evidence is needed on how to reach men who are least likely to engage with traditional services. Community-led organisations sit directly within that agenda. They include pie clubs, walking groups, yoga classes, peer-support sessions, football clubs, workshops, gaming nights, allotments, drop-ins and other informal spaces where men can arrive through ordinary activities rather than through a referral, diagnosis or formal disclosure. Yet this field remains poorly understood. We still know too little about where these organisations are located, which men they reach, how they build trust, and how policy can support them without undermining the informality and local fit that often make them work.
In an interim report, findings from our work, alongside early findings from ONS evidence and a roundtable held by Centre for Policy Research on Men and Boys (CPRMB) in April 2026 point to a central problem for policy. Male suicide risk is geographically uneven but nationally widespread. Suicide remains a persistent and worsening public health concern in England with rates showing a steady increase for the first time in recorded history since the mid-2000s (Figure 1). Suicide, however, is not always experienced, named or acted on as a mental health problem. It is often concealed under life-related events such as debt, family breakdown, addiction or gambling, revealing that prevention cannot rely only on people entering support through clinical pathways.
Figure 1: Suicide by sex in England, 1981 to 2024
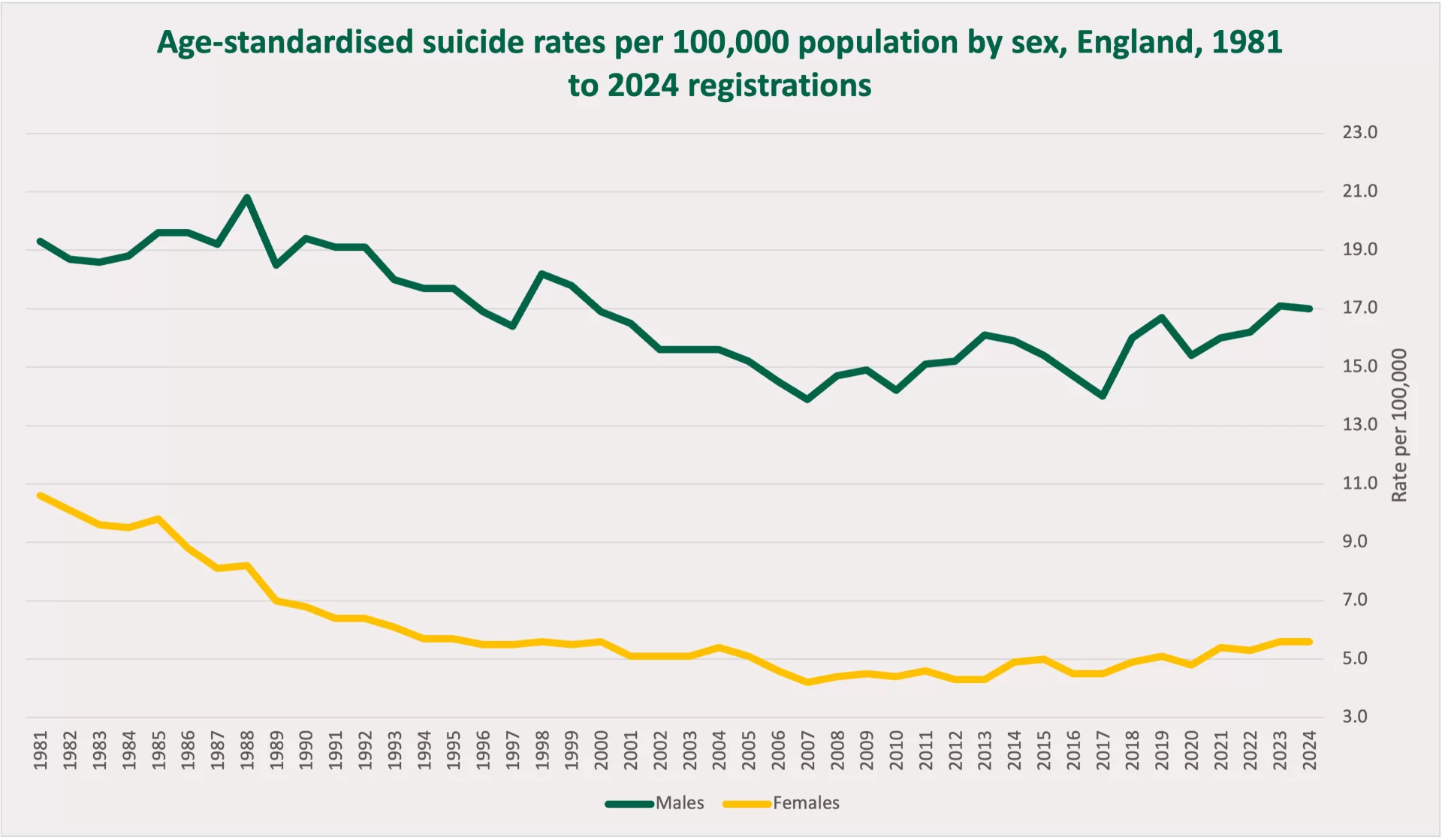
Source: ONS, Suicides in England and Wales dataset, 3 October 2025, Table 1.
The project’s England-wide mapping is an attempt to make this informal prevention infrastructure visible. It has so far identified 2,082 visible community-led, non-clinical interventions for men’s mental health and wellbeing (Figure 2). The map does not claim to be a complete register, but the emerging picture is important. These forms of support are visible, but they are not evenly distributed. Read alongside suicide rates and deprivation, the picture is one of partial overlap rather than clear alignment. There is no simple pattern in which more visible organisations correspond to lower suicide rates. Nor does deprivation reliably predict where community-led provision is most visible.
Figure 2: Community-led, non-clinical interventions per 100,000 population and age-standardised suicide rates, 2022–2024, by local authority
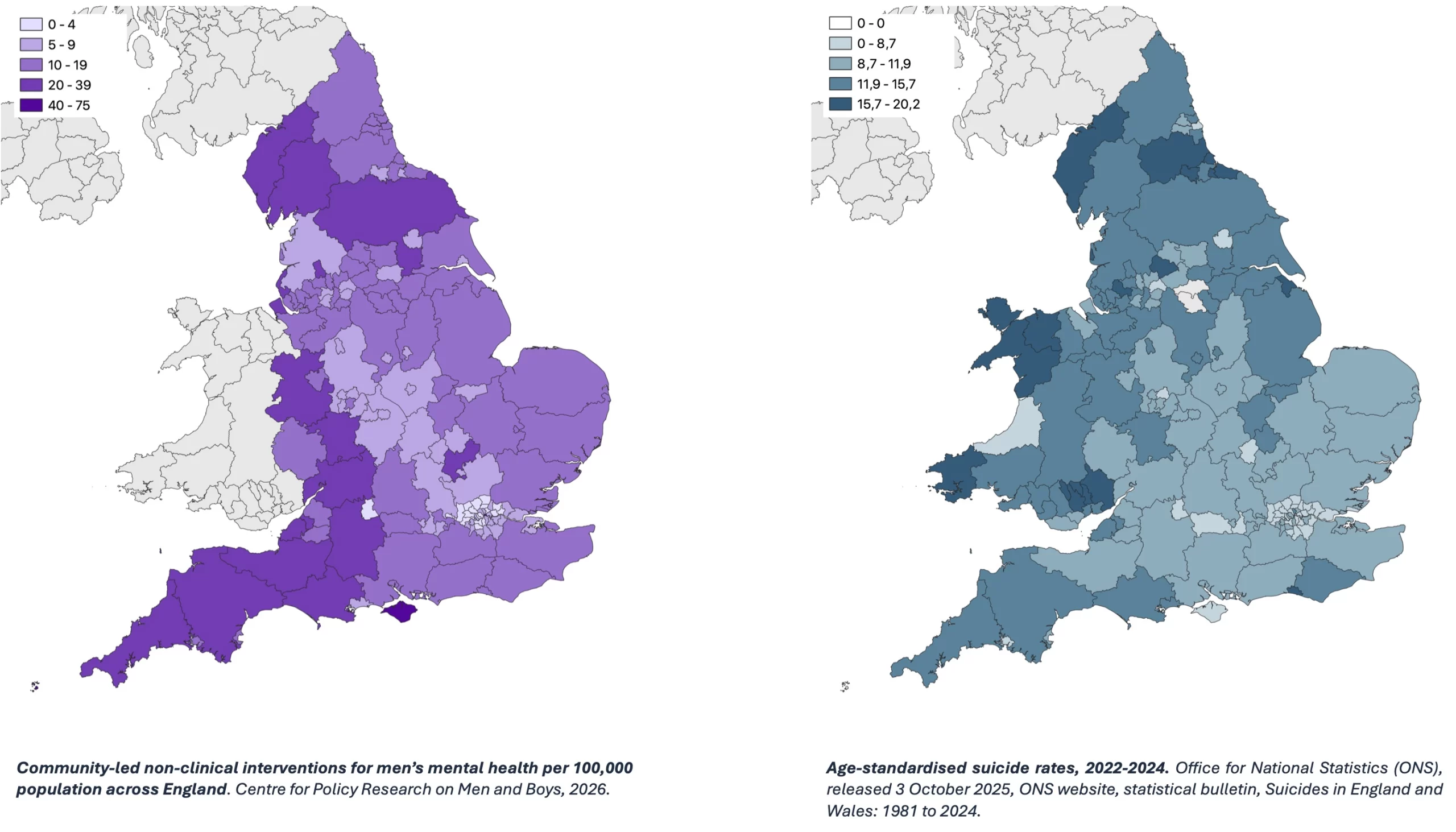
The stronger conclusion is that England has a geography of structural need and a separate, more contingent geography of community response. Sometimes they overlap; often they do not. In parts of the North East and South West, higher suicide rates appear to sit alongside relatively dense visible community-led provision. In other regions, including parts of the West Midlands and South East, visible provision is still present, but many areas sit in lower suicide-rate bands.
The policy task is therefore to understand where support ecosystems are thin relative to need, where stronger local ecologies have emerged, and what kinds of provision are proving effective, for whom and under what conditions.
Redefining outcomes and scaling
Many community-led organisations work because men do not have to arrive through the language of mental health. They can come through sport, walking, cooking, making, gaming, peer groups, workplace settings or informal conversation, and only later begin to talk about what is happening in their lives. This matters for how outcomes are understood. In suicide prevention and men’s wellbeing, the aim is to prevent deaths and reduce serious harm. These outcomes, however, are often not immediate, attributable or easy to count since prevented crises are hard to record precisely because they did not happen. The changes that community-led organisations can most realistically evidence are often indirect and preventative: reduced isolation, stronger connection, renewed purpose, improved help-seeking, trusted peer relationships, safer routes into further support, and stronger organisational capacity. This means developing proportionate evidence. Outcome measures should be co-produced with organisations and participants, sensitive to organisational stage and capacity, and designed as a learning framework rather than simply a reporting framework. The point is to build a common language that policymakers can use without forcing small organisations to measure the wrong things, in the wrong way, at the wrong time.
The research is therefore moving towards a relational account of scale. For some organisations, growth may be appropriate: more sessions, more volunteers, more sites, or a stronger referral relationship with local services. For others, the right form of scale may be depth rather than expansion: becoming more stable, safer, and more resilient. Appropriate scaling may mean enabling local people and organisations with credibility in their own communities to create their own versions of support, shaped by local culture and need, rather than replicating a model designed somewhere else. It also implies a different way of thinking about investment. Funding, evaluation and commissioning should help organisations strengthen what they already do well: supporting leaders, volunteers and trustees; improving safeguarding and governance; sharing practical knowledge; reducing administrative burden; and creating routes into wider support when needed.
Scale, in this sense, is a question of whether local ecosystems become more capable of recognising distress, holding people in moments of difficulty, and helping men move towards further support before crisis point.
Policy and prevention
For policy, the opportunity is to support this field by making it more visible, more sustainable and more transparent without making it less trusted. Many community-led organisations work because they are not experienced as statutory services. Men can attend without a referral, a diagnosis, a formal disclosure or an identity as a patient. This low-pressure quality is not incidental to their effectiveness; it is often the condition that makes engagement possible.
That creates a difficult task for government, commissioners and funders. Community-led support cannot simply be absorbed into the formal mental health system without changing what it is. But nor can it be left to survive through fragile funding, volunteer exhaustion and opaque local opportunity. This is where the prevention agenda becomes concrete.
Preventing crisis is not only about creating more clinical capacity at the end of the pathway, important though that remains. It is also about strengthening the places, relationships and routines that allow distress to be recognised earlier, held for longer, and acted on before it becomes acute. A national men’s health agenda will only succeed if it understands these community settings as part of the infrastructure through which prevention happens. Effective support needs to be shaped by national goals but rooted in local realities.
The next phase of the CPRMB project will deepen this evidence by combining the national mapping with qualitative work in partnership with selected organisations towards a co-produced outcomes framework to understand what kinds of support work, for whom, in which places, and under what conditions.
If policy is serious about moving from sickness to prevention, it needs to understand, support and sustain the local infrastructures where men are already beginning to reconnect.
Photo: Rocker Pier in Sunderland, where Space North East brings men together for weekly walks to combat depression, loneliness and anxiety.
The views and opinions expressed in this post are those of the author(s) and not necessarily those of the Bennett School of Public Policy.




